
One month on, the Ebola disease outbreak is outpacing the response effort. No one knows the true scale or exactly where the disease is spreading in DRC. What we do know is that most treatment centres in Ituri province are overwhelmed; many of our patients arrive at a late stage of the disease, and the majority were never identified or monitored as contacts before seeking care.
Kate White, emergency medical coordinator for MSF in DRC
The disease is spreading across Ituri, North Kivu, and South Kivu provinces in eastern DRC, with Ituri accounting for nearly 95 per cent of the cases. The response, led by the Congolese Ministry of Health and supported by several international partners, is being put in place in the affected areas. Unfortunately, insecurity makes reaching certain communities difficult, and even in more stable areas, efforts to detect cases, test patients, identify contacts, and monitor transmission are insufficient. In neighbouring Uganda, 19 confirmed cases have also been reported by the health authorities.
Congolese health authorities officially reported more than 650 confirmed cases and over 130 deaths. However, MSF warns that these figures likely represent only part of the picture.
Testing remains one of the most significant weaknesses in the response, despite recent improvements in laboratory capacity and the arrival of hundreds of mobile test kits in eastern DRC, designed specifically for the Bundibugyo virus. Many communities, especially those affected by ongoing insecurity, still have limited access to these kits, while treatment centres continue to face significant delays in receiving laboratory results. Without faster and more widely available testing, we will struggle to detect cases early enough to contain the outbreak.
White
In areas where the outbreak is unfolding, millions of people have already been living with decades of active conflict, repeated displacement, chronic gaps in healthcare, and a limited humanitarian response. These conditions severely hamper response efforts and create an environment in which the disease can spread more easily.
In Ituri, where MSF has been present for decades, we have observed fear and mistrust among communities, with some being wary of the sudden arrival of Ebola response teams.
Setting up activities and explaining the disease is not enough to build community trust - people’s concerns need to be listened to, and communities should help shape the response.
Frederic Lai Manantsoa, emergency coordinator for MSF in DRC
For many communities, the outbreak is just one of several health emergencies that have been inadequately addressed for years. Maintaining access to routine healthcare is just as important as controlling the outbreak itself to save lives.
Pregnant women still need maternal care, children still need vaccinations, and patients still need treatment for malaria and cholera. Maintaining access to routine healthcare also helps support Ebola disease surveillance among communities.
White
Although the number of confirmed cases reported in North Kivu and South Kivu is relatively low, they face many of the same challenges around surveillance and testing. In North Kivu, there is only one laboratory to test blood samples, and they take several days to process. Since there is no automated system for sending them to healthcare facilities, it can sometimes take almost a week to get results.
Alongside direct patient care, MSF is also sending teams to more remote and insecure areas to strengthen detection and response capacity where alerts have been reported.
This outbreak can still be brought under control, but the window for action is narrowing. Diagnostics, surveillance, access to care, and community engagement must be urgently strengthened. We urge authorities, and all stakeholders involved in the response, to do everything possible to facilitate the movement of health workers and supplies, and enable a response that matches the scale of this crisis.
Lai Manantsoa
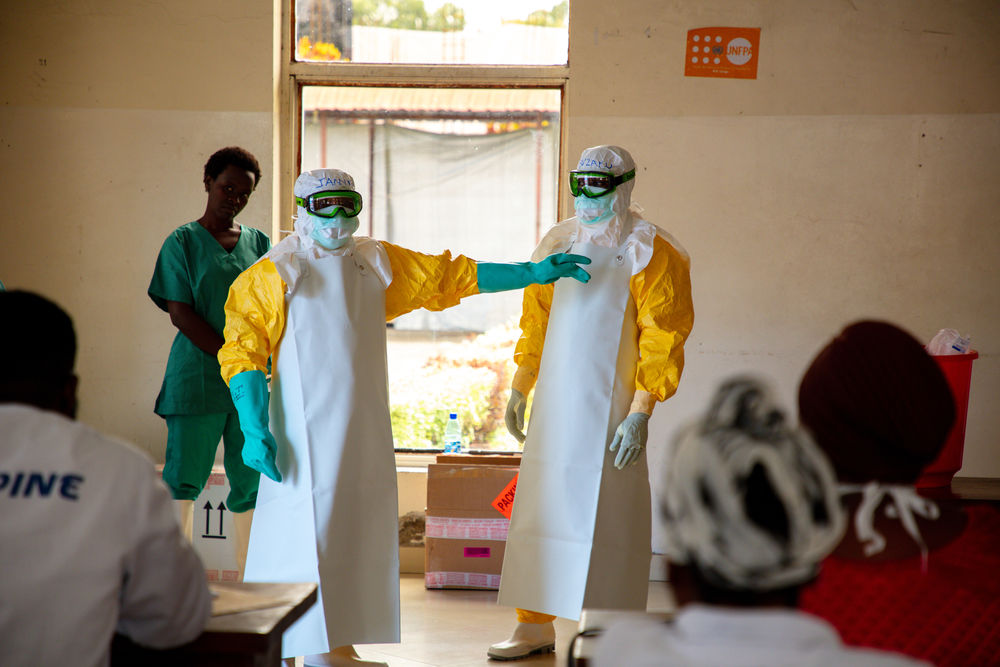
Since the beginning of the outbreak, MSF teams in Ituri, North Kivu and South Kivu have established Ebola treatment centres in Bunia, Mongbwalu, Komanda, Goma, Bukavu, and Lwiro, and we are preparing more isolation and treatment facilities across the three provinces. MSF has reinforced infection prevention and control measures in the health facilities we support. We are also carrying out a wide range of critical activities, including engaging with communities, supporting surveillance activities, training health workers in infection prevention and control, supporting on safe and dignified burials, supplying health facilities with equipment and medicines, and helping to ensure continuity of essential healthcare services beyond the Ebola disease response. Hundreds of tonnes of equipment and medicines have been shipped from Kinshasa and abroad, and nearly 600 staff are currently involved in MSF's Ebola disease outbreak response.
In parallel with our support for the Ebola outbreak response, MSF remains committed to providing impartial medical care to people across DRC, where we work in 16 of the country's 26 provinces. Our teams respond to the needs of people affected by conflict, violence, displacement, and disease outbreaks. Key activities include surgical care for the wounded; treatment of malnutrition; HIV and tuberculosis care; reproductive health services; paediatric care; malaria prevention and treatment; disease outbreak prevention, surveillance, and response; and mental health support. Our teams are also currently responding to other preventable disease outbreaks, including cholera and measles.
MSF is an independent, neutral, and impartial medical humanitarian organisation that provides emergency medical care to people affected by armed conflict, epidemics, natural disasters, and exclusion from healthcare.