The long road to herd immunity
Borderline
01 May 2021
The Long Road to Herd Immunity
From the Executive Director
The Long Road to Herd Immunity
A vaccine injection takes just a few seconds. But it protects us against what is otherwise a very dangerous disease when the antibodies are produced. If the majority of a population gets vaccinated, herd immunity can be achieved. Unfortunately, people in so many places in the world have to go through a lot for these few seconds.
I remember the year I visited an MSF field project in Democratic Republic of Congo, when the emergency team had to respond to one of the measles outbreaks by conducting a mass vaccination campaign in the Lubunga district. I realised then that no matter how well-prepared we are, we still have to cross a series of hurdles — customs, regional administrations, weather, people's perception of vaccines and so on. Overcoming these difficulties requires months or even years of effort. That's why each successful jab is a wonder to me.


Because of this first-hand experience, the title “The Long Road to Herd Immunity” of this issue of Borderline reminds me of all the bumps in the road. In the COVID-19 pandemic, when vaccine doses are still far too few for everyone, the wonder of successful jabs seems even harder to reach. In many countries, health systems have been heavily hit and the recent experience in Brazil and India has been devastating. In some places, where routine vaccination campaigns have been put off, other diseases are emerging and spreading again. If one day we can get to herd immunity here in Hong Kong, can we alone really escape from the virus?
How long really is the road to our herd immunity? Let's have a glimpse.
Jenny Tung
Executive Director, MSF Hong Kong

COVID-19 vaccine: Scarcity means priority groups first
Crisis in focus
COVID-19 vaccine: Scarcity means priority groups first
On 11 March 2020, the World Health Organization (WHO) declared COVID-19 a pandemic. Since then, scientists around the world have been developing vaccines faster than ever before to stop the disease from infecting yet more millions of people. As of 12 May 2021, with over 100 million cumulative cases and 3 million deaths, we have six versions of vaccines approved by WHO for emergency use. Despite the huge progress, the quantity of COVID-19 vaccines, medical tools, and therapeutics currently available are still far from sufficient to deal with the pandemic, especially when manufacturers are struggling to cater for the huge global needs. This harsh reality of scarcity will not change very rapidly, and the question at this very moment is how to make the very best use of the limited resources to protect those who are the most vulnerable.
Priority to the high-risk groups



They are the people at the highest risk of getting the disease or developing severe symptoms when infected. The WHO therefore recommends vaccinating these groups of people before others, with approved vaccines that are largely safe and effective, in order to reduce mortality and keep health care services running. The idea of extending the vaccination campaign to lower-risk groups in some countries before giving it to the high-risk groups everywhere undermines the recommendation. And now it's not only an idea; it is a development we are all seeing.
A reality crueler than the vaccine scarcity
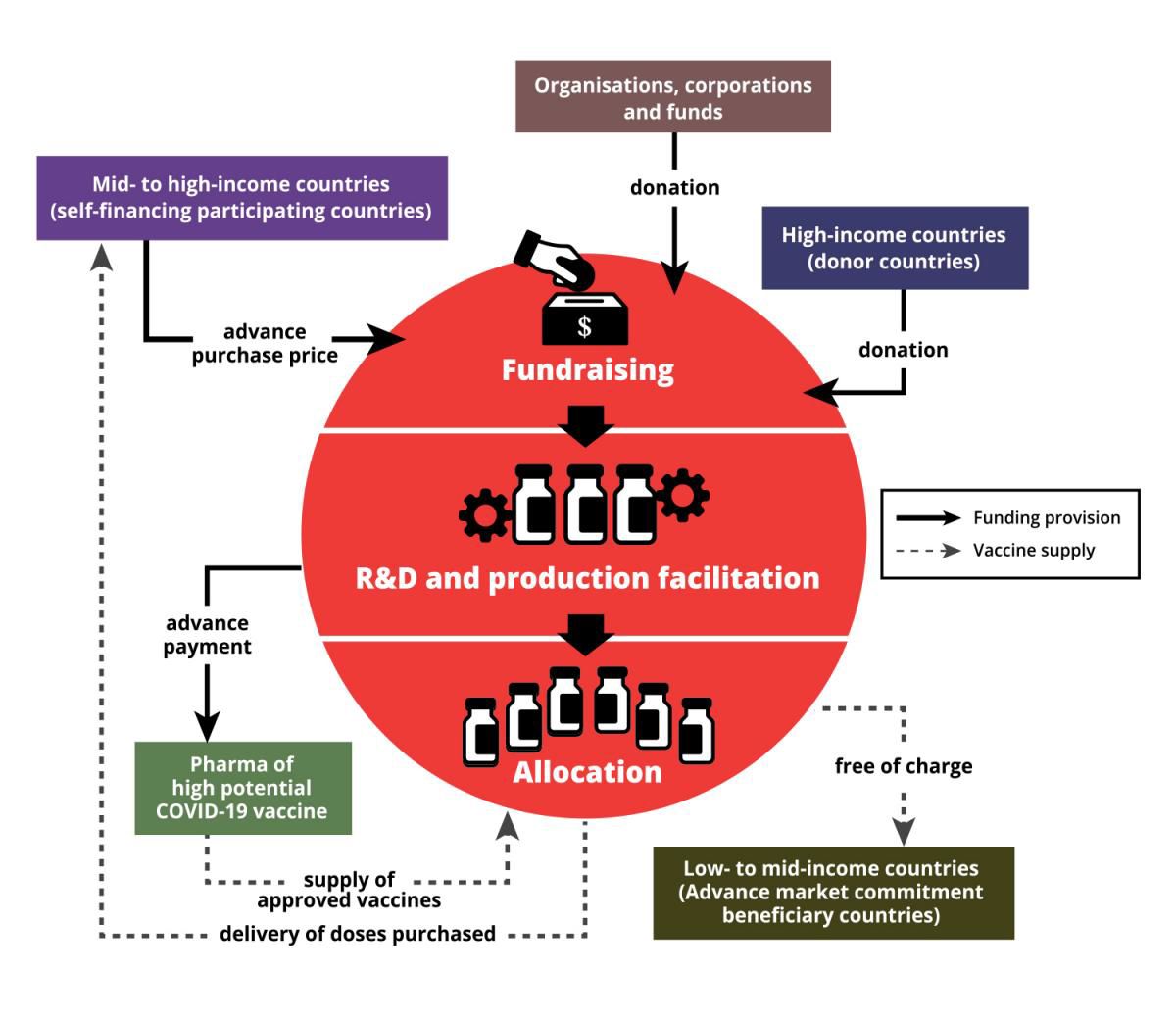
With the intention of helping equitable global access to COVID-19 vaccines, WHO, Gavi, the Vaccine Alliance and the Coalition for Epidemic Preparedness Innovations (CEPI) jointly initiated the COVID-19 Vaccines Global Access (COVAX) Facility last year. COVAX aims to help countries protect their people who are at the highest risks regardless of how rich or poor the country is. The concept of COVAX is a bit of a mixture of the ideas behind crowdfunding platforms, group buying and suspended meals, but of course, it is much more complicated than that. It's more than just a funding instrument, as it also aspires to regulate the prices of approved and licensed vaccines. Below is our attempt to explain how COVAX works:
COVAX is the lifeline for many developing countries in this pandemic, because it's a formidable task for them to compete with richer countries for enough vaccines through bilateral agreements. The success of COVAX hinges solely on global solidarity, especially a show of strong commitment from high-income countries. But this solidarity is yet to be realised.
Access to COVID-19 Tools Accelerator (ACT-A) is a global collaboration to speed up the development, production and equitable access to new COVID-19 diagnostics, therapeutics and vaccines, and COVAX is its vaccine pillar.
"COVAX was built on the understanding that bilateral agreements would happen. What the problem has been is the extent of these bilateral deals," said Amanda Harvey-Dehaye, leader of MSF's ACT-A task force.
"Countries who have met all their needs uniquely through bilateral deals, and therefore don't need COVAX doses too, are supposed to inject money into COVAX anyway. This would leave COVAX able to negotiate with pharmaceutical companies for vaccines for the lower income countries this mechanism subsidises. But this didn't happen enough, and through all their bilateral deals, a few wealthier nations have hoarded up a vast part of the available supply – which is anyway less than hoped for, given the production problems and manufacturers over-committing," Amanda added.
Major obstacles faced by COVAX

As of March this year after the G7 leaders committed USD 4.3 billion to ACT-A, it still faced a funding gap of USD 22.1 billion to reach the target for 2021, and COVAX alone was USD 3.2 billion short. The disparity of vaccine supply also undermines COVAX's efforts for equity amongst nations through a pooling of resources. According to WHO, more than 800 million vaccine doses have been administered globally as of mid April this year, and over 83% of them have gone to high-income or upper middle-income countries, while low-income countries have received just 0.2%. Some wealthy countries and regions, including Hong Kong, have snapped up more than they need to create herd immunity in their societies. Quite a number of them even purchased more than double the number of vaccine doses that their entire population needed.
Countries like the United Kingdom and the United States of America started vaccinating their population in mid-December last year, while COVAX only managed to commence the first batch of vaccine delivery (doses for 3% of their populations) to low- and middle-income countries in early March this year. Some of those countries, with more than enough vaccines, had already begun to extend their vaccination campaigns to their lower-risk groups whilst many developing countries are yet to complete or even start vaccinating their high risks population.
Kate Elder, senior vaccines policy advisor of the MSF Access Campaign explains that it's not just about fairness to vulnerable and neglected people in developing countries. "Even if you are just looking at it from a public health perspective, if you can prevent the disease from circulating, it's to everybody's benefit. It makes total sense of saying equity of access of COVID-19 vaccines is critical." She further explained that the emergence of recent virus variants in the midst of global transmission becomes more worrying, and as we are all part of the global community, no countries are likely to be spared. She cited the United States, the country she lives in, as an example. "If there is another variant of the virus that is replicating in some other parts of the world, eventually it's going to make its way here to the United States. So, there is no point in herd immunity in one country if you're not looking to achieve equity of immunization across the globe."
Global spirit of solidarity is needed to put a halt on COVID-19

The spirit of solidarity can be as simple as donating vaccines to developing countries that critically need them for their vulnerable groups. Some governments like the UK, Canada, France and Norway promised to share vaccines with developing countries, but it's not clear when the donation of surplus doses will begin, and urgent supply of COVID-19 vaccines are needed now. If these countries will only donate doses after they have completed inoculating their entire populations, the world could be in a much worse position as the virus continues to circulate.
"It would be indefensible if some countries started to vaccinate their lower-risk citizens while many countries in Africa are still waiting to vaccinate their very first frontline health workers,” said Christine Jamet, MSF director of operations. “This totally goes against the World Health Organization's equitable allocation framework."
There are other dangerous behaviours that could damage everyone. Blocking the export of vaccines and their raw materials and manipulating intellectual property rights to monopolise life-saving biomedical or medical technologies may prolong the pandemic and put even more lives at risk.
For example, South Africa and India sponsored a proposal regarding the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) in the World Trade Organization (WTO) last October. It proposes to allow WTO members to temporarily waive the intellectual property rights on medical tools and technologies for COVID-19 preventions and treatments if they need to. However, high-income countries have been standing in the way of the waiver proposal and the discussion went into an impasse. Only when the US government changed its position to support the waiver on COVID-19 vaccine (Note: not on other COVID-19 medical tools) in early May, some countries that opposed the proposal showed willingness to further discuss it.
This proposal may not be a silver bullet to rectify the current situation right away, but it is indeed a huge step that could help the availability of medical tools and technologies for COVID-19 in the near future. Many other developing countries and civil society organisations around the world, including MSF, hope that the TRIPS waiver will be accepted and approved by all the member states in the end.
Only when all countries can take part in research, development and production to let diversity flourish, will there be a chance for us to bid farewell to the scarcity of lifesaving medical supplies and tools, and thus the COVID-19 pandemic.
Why are vaccines related to cow?
Diving in Details
Why are vaccines related to cow?

We need to go back to the deadly infectious disease of smallpox when we talk about vaccines. A method called "variolation" was used as much as few hundred years ago, where people were exposed to material from smallpox pustules in the hope of getting protection from the disease. However, this practice posed risks and people might die from it.

In the 18th century, an English doctor, Edward Jenner, noticed that milkmaids sometimes caught the mild disease of cowpox from their herds and then seemed to be protected against smallpox.

Jenner tried inoculating - or deliberately infecting - an eight-year-old boy with cowpox pustules. After he recovered from the mild disease, Jenner exposed him to smallpox. The boy resisted the infection; Jenner had made him immune to smallpox. The doctor then carried out more experiments and published his findings. His discovery pioneered the development of modern vaccination.
The importance of mass vaccination campaigns
Perspective across borderlines
The importance of mass vaccination campaigns
Humans have been living with infectious diseases, some quite deadly and contagious for centuries. People have weathered severe health crises – from smallpox, Ebola, measles, cholera – and one of the turning points was the discovery of vaccines. Within living memory, smallpox, a highly contagious disease and one of the most brutal killers in human history claimed countless lives. It was finally declared eradicated in the 1980s because of the effectiveness of smallpox vaccine. Nowadays, a range of vaccination campaigns are continuing to safeguard public health worldwide.
"Our medical teams have seen many times how a vaccination campaign has stopped an outbreak. It is kind of a miracle, that in 10 to 14 days, you stopped receiving patients," said Miriam Alia, MSF vaccination and outbreak response advisor. MSF has learnt from experience that when there are outbreaks like measles, meningitis, cholera and diphtheria, mass vaccination campaigns help tackle the transmission. It is also an effective preventive measure against outbreaks in crowded, constricted camps where people take refuge during crises.

While vaccines are effective in managing outbreaks, such protection is not readily accessible to everyone. Miriam recalled an example of her colleagues working in town of Mingala, Central African Republic (CAR) that she supported in the headquarters in 2019. The town was under siege for more than two years and our medical teams were prevented from getting to the trapped communities. After a year-long negotiation, the team was finally allowed to enter and managed in only a few days to vaccinate almost 1,000 children born during the siege against nine diseases. It's such an important first step that protects against so many hazards.
Not only kids were vaccinated, pregnant women also received their jabs against tetanus and diphtheria and provided curative consultations and antenatal care. "They told the team they had not seen a doctor for more than two years. They were really pleased that we vaccinated their kids. And it was telling that they knew very well the importance of the vaccination."

Today, mass vaccination campaigns against the diseases that kill the most children under five were disrupted not only by challenges posed by conflict and security issues where MSF works, but also by the COVID-19 pandemic. Our field teams have been trying to respond to the current pandemic and to deal with existing medical humanitarian needs, which certainly includes preserving the continuity of care for patients affected by other fatal diseases.
"Due to lockdowns, the transport of medical goods was very difficult," said Miriam. "Even when cargo planes are available, they are dedicated to supplies for COVID-19 response, such as personal protective equipment." Other supplies that fall outside of the pandemic response are not a priority, making vaccines for other diseases even less accessible to people who need them most. Across Africa, at least 110 planned vaccination campaigns by Ministries of Health have been delayed, and some of them were yet to be implemented at the beginning of this year. These measures were taken to avoid overcrowding that would increase COVID-19 infections.
Miriam reveals that MSF has adapted a new approach in the Democratic Republic of Congo in order to reach children and communities safely. Measures had to include reducing the number of people to be vaccinated by each team on each day and maintaining social distance in the queue. We also went door-to-door to give oral cholera vaccines in Niger to try to keep people protected from the disease. Our teams implemented these measures even before the World Health Organization issued its own, similar recommendations for conducting vaccination campaigns in COVID-19 settings.

However, the pandemic continues to slow down our ability to vaccinate more children. Our medical teams are concerned with the surges of measles infections we are seeing in countries like Mali, Niger and Democratic Republic of Congo due to children being left unvaccinated. It's inevitable that vaccine-preventable epidemics will show themselves soon.

Access to vaccines against COVID-19 and all other diseases are equally crucial. All of us will need to adapt to this new normal and carry on effective vaccination campaigns to protect more people from the threats of epidemics.
Measles Vaccination Campaign in Timbuktu region, northern Mali
Witnessing through the lens
Measles Vaccination Campaign in Timbuktu region, northern Mali
In September 2020, MSF alongside the Ministry of Health undertook a three-stage campaign targeting over 60,000 children aged between 6 months and 14 years in the region. In addition, all children and the people accompanying them were screened for COVID-19 and treatment assured for suspect cases. The campaign targeted 12 health zones, some easily accessible in urban areas and others outlying areas reached by dug-out canoe.
© MSF/Mohamed Dayfour