The many faces of Violence
The high levels of violence in Syria have shocked the world in recent months and MSF is struggling there to treat some of the victims of the conflict. But we see terrible symptoms of much more hidden and neglected violence in many parts of the world, one of which we would like to highlight in this issue of Borderline.
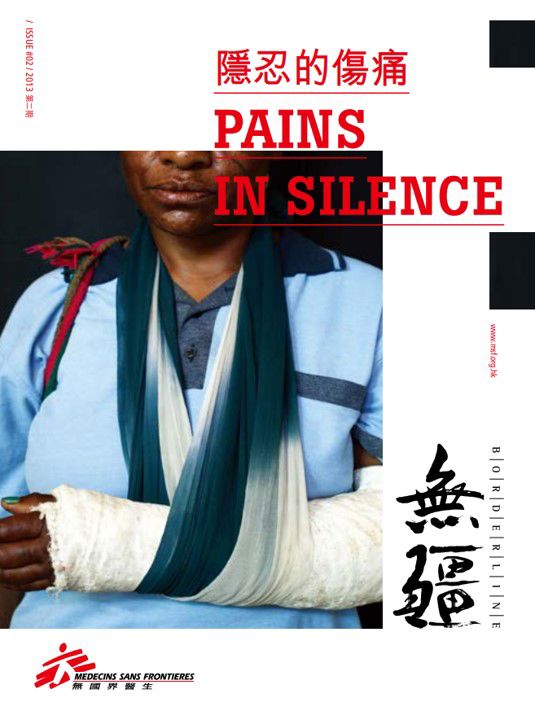
In Papua New Guinea (PNG), women suffer from the consequences of family and sexual violence every day, from visible physical wounds to less visible but equally damaging psychological trauma. However, many of them prefer to keep things hidden, often because they have nowhere to go and no one to care for them. MSF has worked in PNG since 1992 and has witnessed how violence is ruining people’s lives. We are there not only to provide victims with the essential medical care, but also to push for policy change. The government and civil society should do more to ensure specialised services are available in each province. Women should be able to find medical teams who will care and help to heal their scars.
In Somalia, violence has also forced MSF to make the very difficult decision of withdrawing from a country where MSF was present since 1991. Somalia has long been one of the most dangerous places for humanitarian aid workers, their local colleagues and patients. Despite the numerous compromises MSF made in response to the unparallel levels of risk, the constant series of attacks, including abductions and the killing of 16 of our staff, showed the absence of a basic level of respect for humanitarian action in the country. In many cases, the violence is tolerated, condoned or even supported by those who should be protecting us. This pervasive and permitted violence pushed us to beyond our limits and ultimately forced us to leave the country. The Photo Feature will present our 22 years of work in Somalia, where humanitarian assistance is still today greatly needed to help people caught in this terrible conflict.
Amidst all the challenges and setbacks, MSF remains strongly committed to providing healthcare to those trapped in all forms of violence. We will continue to push for further access to those in need, for more protection for our doctors but also for those they treat. This will not be possible without your help and support.