For Afghanistan, a country which has been trapped in war for so many years, 2014 is a critical year, with the presidential election in April and the withdrawal of the US army by the end of the year. Claims and reassurances have been made about the achievements of the international community in rebuilding the country, including the provision of healthcare. MSF's own study though finds that Afghan people are still facing multiple challenges in getting treatment.
Last year, MSF conducted six months of research, interviewing 800 patients and their caretakers in four distinct regions. One in every five of the patients had a family member or close friend who had died last year due to a lack of access to medical care, while 40% of patients faced fighting, landmines, checkpoints or harassment on their journey to MSF hospitals.
Barriers to healthcare
Distance, insecurity and high cost are the main obstacles. 12% of interviewees said it took more than two hours to get to the hospital. Some people, too afraid to go out and find a doctor in the dark, were forced to watch over their sick or injured relatives throughout the night, hoping they would survive until morning to bring them to a hospital.
Most interviewees live in poverty, with each household surviving on US$1 per day but having spent an average of nearly US$40 on a recent medical consultation. They also need to pay for transportation, accommodation and other costs, which push many into debt or force them to sell their few possessions.
Some public hospitals, while promising to provide free healthcare, lack quality medical staff, facilities and drugs. Waiting times are too long and the referral system is weak. A 33-year-old woman from Helmand province said, “The government clinics are always crowded with sick people. You have to bribe the doctors to be seen. They don't really care about the patients. They are just waiting in their office for the day to end so they can go home.” Many patients prefer to travel greater distances, at significant cost and risk, to seek care from private hospitals. But interviewees also spoke of misdiagnosing and overprescribing from the private practitioners they visited. All the more reason that public health facilities should offer quality care as an accessible and affordable alternative.
Difficulties facing humanitarian organisations
One reason the health system is failing to address peoples' needs is that decisions taken by belligerent governments on where and how to provide assistance in Afghanistan have too often been based on considerations such as stabilisation, counter-insurgency strategies or “winning hearts and minds”, rather than medical needs. Aid was directed towards insurgency-affected areas where international troops were present, while other areas were overlooked.
The consistent insecurity and limitations on access to conflict areas prevent humanitarian organisations like MSF from providing a sustained response. Michiel HOFMAN, the former representative for MSF in Afghanistan, says the only answer is to talk to all sides. “MSF has been able to carve out operational space in Afghanistan through regular, direct, and transparent negotiations with all the warring parties, and complete financial independence from western and Afghan government sources.”
MSF is very concerned that continuing conflict in many parts of the country and a failure to meet rising medical humanitarian needs will coincide with a reduction of interest from international community after the withdrawal of the US army. International donors, aid providers and Afghan authorities must make more efforts to ensure impartial healthcare can be provided to all sick and wounded, while putting aside any considerations other than people's needs.
Afghan women: harsh fate
Statistics show that one in 42 women in Afghanistan is likely to die of issues related to pregnancy and childbirth. The maternal mortality rate is one of the highest in the world.
One reason for this is the dire lack of female medical staff, particularly in rural areas. Many women are reluctant to be examined or treated by male medical staff. And then there are travel and safety fears. “The government clinic in our area is only open until 12 noon. So pregnant women with complications have to wait for the next day until the road is secure.” A resident from Lashkar Gar said. “Most of them die because they can't reach a hospital in time to save them.” What makes things worse is that women in most areas require consent from their husbands to visit a health facility, and usually have to be accompanied by a male relative.
To reduce the maternal mortality rate, MSF has operated a maternity hospital in Khost province since 2012, with an all-female medical team providing 24-hour free healthcare. In 2013, MSF performed nearly 12,000 deliveries in the hospital.
“I've already paid so much to help my daughter. Now I’ve run out of money. I spent it all on private doctors or traveling to them. We came here (to Boost hospital) because it's free. Yet when she was discharged we needed to stay here in the town, near the hospital, to bring her for daily follow-up appointments. So, even though the healthcare here is free, it still costs money for me to stay close to it.”
- A 39-year-old Mullah* from Helmand
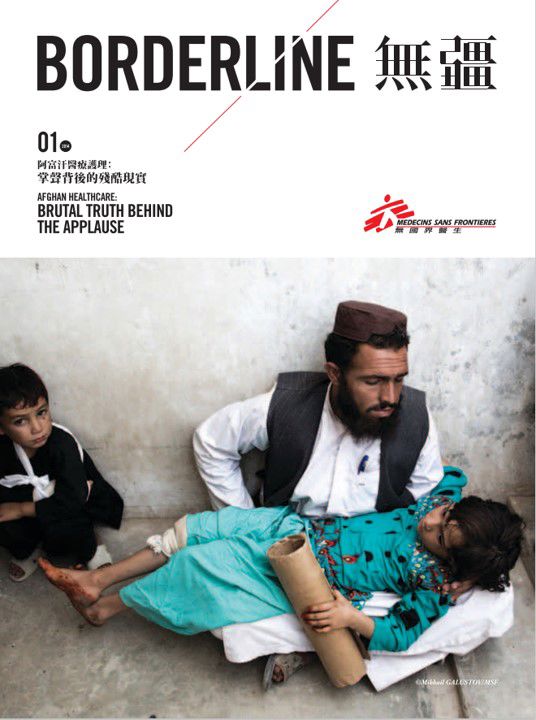
“We can't move at night or all of us would be killed on the road. So, we prefer that they die quickly rather than having to suffer through the night only to die the next day or on the way. This is our reality.”
- A 50-year-old farmer from Kapisa
“In my area, there's just one private doctor and he used to fix tyres. He didn’t study medicine, but has one big medical book in Pashto. When I went to see him with head pains he told me to look up the book myself to find a treatment. That’s not a doctor! How can he treat anyone who is seriously sick?”
- A 22-year-old farmer from Helmand